At Accuray, we are committed to designing radiotherapy solutions that can take on the most complex challenges — while making commonly treatable cases even easier. Our unique, market-changing solutions are designed to deliver radiation treatments across a full spectrum of patient needs, with a global reach that extends our innovative practices worldwide. Our commitment to continued innovation aims to enhance care, improve quality of life, and address diverse healthcare needs around the globe.
0+
systems installed
Treatment systems in
0+ countries
+0% of FY23
revenue invested in R&D
Quality of Care
Deliver precise radiation therapy treatment to ensure optimal outcomes.
Precise robotic treatment as
individual as every patient
Delivers stereotactic radiosurgery (SRS), and
stereotactic body radiation therapy (SBRT),
treatments anywhere in the body with true robotic
precision and integrated, AI-driven, real-time
motion synchronization.
Expands patient-first treatment like no other system in the world
Integrated 3D kVCT and megavoltage CT (MVCT)
imaging for advanced image-guided
intensity-modulated radiation therapy (IG-IMRT)
and 3D conformal radiation therapy (3DCRT).
Precise robotic treatment as individual as every patient
Delivers stereotactic radiosurgery (SRS), and stereotactic body radiation therapy (SBRT), treatments anywhere in the body with true robotic precision and integrated, AI-driven, real-time motion synchronization.
Expands patient-first treatment
like no other system in the world
Integrated 3D kVCT and megavoltage CT (MVCT) imaging for advanced image-guided intensity-modulated radiation therapy (IG-IMRT) and 3D conformal radiation therapy (3DCRT).
A peer community dedicated to advancing radiosurgery and radiotherapy
Join our thriving Accuray users’ community, gaining free access to a platform to connect with peers, exchange experiences, and keep up-to-date with news and developments in your field. You’ll also have access to a wide range of training opportunities to ensure you stay informed about the latest advancements. Connect, exchange, and learn with us.
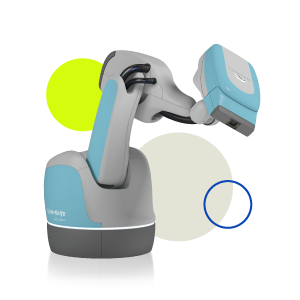
The CyberKnife S7 provides quicker treatment time for patients; therefore the easier it is for patients to tolerate, and their overall experience of treatment is optimal. CyberKnife S7 provides speed, precision and motion synchronization.
These results [PACE B] will change the way certain types of prostate cancer are treated. Using SBRT to deliver treatment would mean that patients could be spared numerous visits to hospital, allowing them to get back to their lives sooner
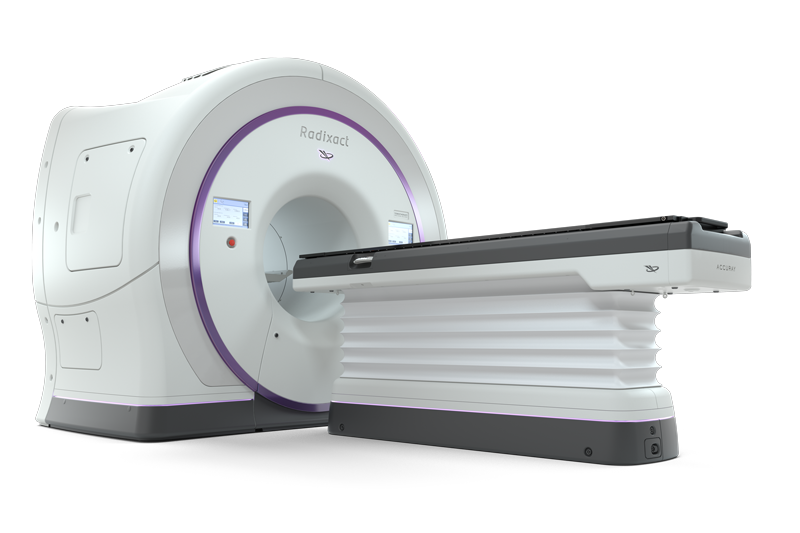
The Radixact® System along with ClearRT™ from Accuray has the potential to change the field of radiation oncology. This 'breakthrough' imaging technology will allow teams to improve care via better visualization of tumors while also shortening treatment times.
Previous
Next
What's new
Insights, research and perspectives from the leading edge of cancer treatment.
Industry-leading service to support your ongoing success, from speedy install and optimization, to proactive monitoring and unrivalled on-site service, to smart upgrade paths to keep your system at the leading edge.
From robotic to helical radiation therapy delivery, we invent unique, market-changing solutions that are designed to deliver radiation treatments across a full spectrum of patient needs.
Accuray is expanding radiation therapy: our products can deliver it accurately, precisely and effectively, from oncology to neuro-radiosurgery and beyond.